Debate, article: How long will the well-intentioned guardian state continue legitimizing torture in psychiatry?
Sorry for poor quality of this Google translation:
Norway should ensure that police and relevant health personnel receive training in the Convention Against Torture. UN Committee against Torture in 2012 CAT/C/NOR/CO/6-7
Walter Keim, retired Assistant Professor, tel.
45435004
Almbergskleiva 64
NO-6657 Rindal, 12. February 2017
Open letter to the Directorate of Health, Knowledge Centre, Institute of Public Health, Medicines Agency, Patient Safety Program, NORMENT, Experience Expertise
Cc: Humania FOUNDATION: For a human mental health, Jaakko Seikkula, Jan Ivar Røssberg, Npf Quality Committee, Medicine Free Offer, Npf, Psychological Association
Referring to the conference at the House of Literature 8th February at 17-21. What is the knowledge base for treatment with or without the use of psychotropic drugs? (1) of Humania FOUNDATION, where Fellesaksjonen, Ivar Røssberg, Robert Whitaker and Jaakko Seikkula gave contributions.
Beforehand Røssberg got documentation of the low evidence of Paulsrud committee and if it overrides the UN Special Rapporteur on Torture's prohibition ( "ban") of all forced medication.
The award-winning science journalist Robert Whitaker cited researchers who have examined the long-term effects of psychiatric drugs. This group will in many cases experience more frequent readmissions and poorer functioning compared to patients without long-term medication (4). This recognition is now mainstream among leading scientists (1).
Regarding symptoms are long-term studies that psychotropic drugs that withdrawal leads first to a little increase but then falls symptoms drastically. In the long run leads psychotropic drugs frequently to psychotic symptoms (2).
In studies of short-term effects often there is not a pure placebo group without medicine, but the “placebo group” consists of patients haven taken psychotropic drugs e. g. a year and then taken off the drug, i.e. withdrawal symptoms are included(Cochrane.org 2011) (2). Therefore, these studies are not real. Thus PAULSRUD committee alleged low positive treatment effects are even lower possibly erased.
While before 2011 can excuse psychiatry being a victim of its at dwelling myths, it must now be assumed that continuing as before is indefensible. Røssberg is an example where delusions that one "knows" about the good effect seems not correctable through information.
Psychiatry's tale that everything was so much better after the introduction of psychotropic drugs are stripped as myth. Studies in the United States, Norway and other countries shows that hospital discharge was higher before the introduction of psychotropic drugs. Which is not surprising, as it is in line with both the alleged short-term effect is undocumented and long-term injuries for many patients documented. Current practice creates more chronically ill than before the introduction of psychotropic drugs (1).
This shows that psychiatric practice today damages more than it helps. To this evidence had psychiatrist Ivar Røssberg only polemic that "Whitaker is the Donald Trump of Antipsychiatry." No separate studies documenting evidence of antipsychotic medications were shown. Can contempt of scientific knowledge remonstrates clearer? Almost all organisations of the common organisation of drug-free offerings were difamet as antipsychiatric.
Røssberg object to drug-free treatment (only about 3% of the beds in Health North) to ignore that there are studies on off medications treatment showing evidence. Treatment without demonstrable effect, must according to him happen outside the public health system, but evidence that antipsychotic forced medication injuries ignore Røssberg (1).
Røssberg claiming "antipsykotics are effective," but did not define what he means is effective: symptom relief and / or recovery? He said neither answred questions about Pauslrud conclusion that 5 to 10 patients must be treated to obtain a patient better in a short time frame. Regarding to project TIPS, so he came to that approximately 1 of 3 patients achieved improvement to return to family / job. But TIP has no radominisert double-blind design. Patient groups in 2 different health districts are compared. The possible sources of error are not even discussed.(6)
Patients perspective came especially advocated when Haakon Rian Ueland for Fellesaksjonen for drug-free treatment process began by reading aloud from the blog of Eline, who has a psychosis disorder, is clearly on his own experience of being medicated against their will. Orders of the authorities of off medications treatment was opposed for a long time of psychiatry.
Obviously do not drug-free offer documentation of positive evidence to be better than today's psychiatry when it was documented that the current over medication harm more than it helps. Fellesaksjonen emphasises rightly that the patient's motivation and desire is important because it gives the placebo effect. The documented strong rejection of forced medication however activates nocebo, that negative effect. When positive short-term effect is not documented and occasion. long-term injuries are forced medication ready illegally.
Because drugs reduce the risk of relapse, they are also used prevention in long-term treatment (...)
Against this background, antipsychotic drug treatment recommended as first-line treatment both in acute psychosis conditions and the prevention of recurrence.
The assumption of the prevention of "recidivism" (really too withdrawal) it is even more long-term treatment (creates chronic conditions) is incorrect.
It is tempting to point out that the research confirms patients' scepticism and resistance to medication. However, the well-intentioned guardian state power to psychiatrists with a reality shortcoming regarding the harmful effects and lack of usefulness to forced drugging patients possibly being chronically ill. The argument is that the patients do not know their own best occasion. serious anger disorder.
It is now also clear why the United Nations Special Rapporteur on the rights of persons with Disabilities urges abolishing compulsory treatment: "Dignity must prevail" - An appeal two do away with non-consensual psychiatric treatment World Mental Health Day - Saturday 10 October 2015 "The concept of 'medical Necessity' behind non-consensual placement and treatment falls short of scientific evidence and sound criteria. 'Special Rapporteur on Torture Juan E Méndez oration 4th March 2013 as follows: "States should impose an absolute ban on all forced and nonconsensual medical interventions ... "
Jaakko Seikkula talked about "Open dialogue with families increase item resources for Avoiding Unnecessary medication and improve the outcome in psychotic crises" (3). While Open dialogue presented the result of more than 80% recovery shows TIPS as Røssberg propagated that 70% of participants taking antipsychotics after 10 years, that was dependent on antipsychotics. Supporters of traditional psychiatry of medication see this dependence that is created by the medication incorrectly as evidence that patients need medications and are also due. this wrong perception towards drug-free treatment slots.
On this basis, the Directorate of Health, Knowledge Centre of Public Health. Norwegian Medicines Agency is requested to stop legitimising psychiatry harmful over medication in favour of going in for a knowledge- and research-based accumulation of evidence-based health practice based on informed consent.
Follow-up: Editor of the Journal of the Norwegian Medical Association, The inner conflicts of psychiatry exposed. he debate on drug-free programmes in mental health care concerns the nature of psychiatry – and what it ought to be. http://tidsskriftet.no/en/2017/03/editor/inner-conflicts-psychiatry-exposed
Attachments:
Knowledge base for treatment with or without the use of psychotropic drugs? https://www.youtube.com/watch?v=Vu8i0SeHqjQ h2. https://home.broadpark.no/~wkeim//files/kunnskapsgrunnlaget.html
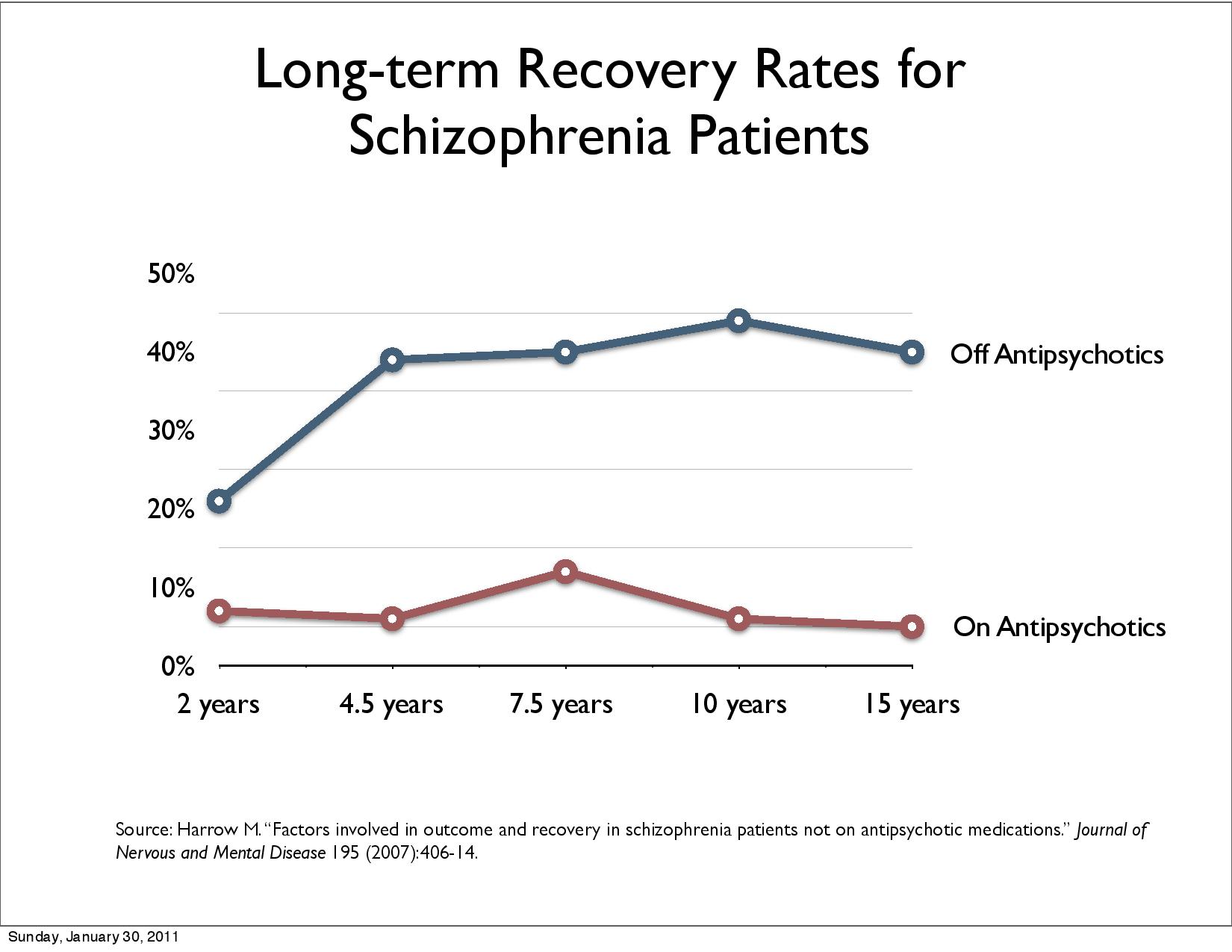
Martin Harrow: Psychiatric Medications and Long-term Outcomes for Schizophrenia https://www.madinamerica.com/psychiatric-medications-long-term-outcomes-schizophrenia/
Open Dialogue — Alternative Care for Psychosis In Finland Developed By Jaakko Seikkula https://beyondmeds.com/2010/01/04/alternative-for-psychosis/
Robert Whitaker. The Case Against Antipsychotics https://www.madinamerica.com/wp-content/uploads/2017/01/The-Case-Against-Antipsychotics-2.pdf
Robert Whitaker. Rethinking Antipsychotics: Recovery Rates and Long-term Outcomes for Unmedicated Patients with Schizophrenia Spectrum Disorders - Litteraturhuset February 17 video, pdf: http://www.stiftelsenhumania.no/2017/02/20/rethinking-antipsychotics-robert-whitaker/
Centre for Research in Evidence-Based Practice (CREBP). Long-term Follow-up of the TIPS early detection in psychosis study: Effects on 10-year outcome – facilitated by Dr Andrew Amos http://www.crebp.net.au/long-term-follow-up-of-the-tips-early-detection-in-psychosis-study-effects-on-10-year-outcome-facilitated-by-dr-andrew-amos/
Walter Keim
Almbergskleiva
64
6657 Rindal, 31. January 2017
Letter to Professor Jan Ivar Røssberg, University Oslo
Copy: Robert Whitaker, Jaakko Seikkula, Humania STIFTELSEN, Medisinfrie Tilbud, Knowledge centre (Kunnskapssenteret), Experience expertise (Erfaringskompetanse), Health institute (Helsedirektoratet), Drug administration (Legemiddelverket)
I refer to the contribution of Jan Ivar Røssberg: «Psychiatric wards without medication: Why is it a bad idea?» conference at Litteraturhuset 8. February kl 17-21 about What is the scientific basis of treatment with or without neuroleptics? of the Humania STIFTELSEN.
As part of the realisation of "patients health service" the ministry of health gave the assignment for «Medication free treatment for psychiatric patients».
Norwegian psychiatric association has not taken position but some psychiatrists criticised the offer as unethical, without evidence an experiment and call it a "gigantic mistake" (see Health minister makes totally wrong choices).
Patients meet the following reality:
Many get not healthy even after many years medication
In fact patients with schizophrenia live 20 years shorter then other people. Nearly all are treated with antipsychotics. (see Responding to the Catastrophic Reduction of Psychiatric Patients’ Life Expectancy, a keynote at WPA XVII World Congress of Psychiatry Berlin 2017)
«Patients and health personnel have different opinions if medicine is necessary. One of the discussions between patients and health personnel is if medicine is necessary for treatment. Normally health personnel holds the opinion that a patient must use neuroleptics, but the patient does not want it.» (Experience expertise 2012:3. Force in Health care. Personnel and dissatisfied patients have different opinions)
Forced treatment can be experienced as trauma, retraumatisation and abuse. «Patient experiences show that forced treatment is experienced as strong traumatic abuse» (Health directorate: Kontroll av tvangsbruk i psykisk helsevern i 2015). The report of Sivilombudsmanns unit for prevention of torture, Kristiansand 7.-9. September 2015 says: “Most patients under forced medication had negative experience e. g. described as «terrible», «cruelly», and «torture».”
«Surveys (see Hammervold, 2009 and Wynn, 2004) show that ”patients experience of physical restrains is characterised of health systems power and patients vulnerability with feelings of powerlessness, loneliness, fear and retraumatisation” (Norvoll og Husum, 2011, s. 23). For those who have experienced abuse earlier, physical restrains may result in very negative consequences not the positive effect, health personnel expects.» (Experience expertise 2012:3. Force in Health care. Personnel and dissatisfied patients have different opinions)
Approx. two third of patients file complaints against forced treatment
There are few alternatives: basically the choice to take medicine voluntarily or forced medication
From a patients perspective questions are:
Patients are interested to become healthy which is best shown by «Number (of patients) Needed to Treat», value 1 meaning that all patients become healthy. Paulsrud committee concluded:
Chapter 9.2.1 Effect on acute psychotic symptoms: «Number of patients to be treated for one extra patient to become better (Number Needed to Treat), from 5 to 10».
Chapter 9.2.2 Effect of maintenance treatment: A meta-analysis of studies comparing effects of second generation antipsychotics and placebo, concludes that the danger of med at danger for relapse is reduced by approx 25 percent. That means that one can prevent one relapse for four patients that are treated for one or two years.»
Compulsory psychiatric care outside hospital (TUD) is used much. According to Zinkler, Martin: Risikobasierte Allgemeinpsychiatrie : Wirkungen und Nebenwirkungen.Recht & Psychiatrie Jg. 32, 2014, Nr. 2, S. 64-68 : Tab., Lit. (2014) 85 patients have to be treated to prevent one hospitalisation.
Are there other research results, which grantee that the law requirement of high probability of positive effect is reached?
After Paulsrud committees report in 2011 the Council of Evidence-based Psychiatry was founded 2014 with focus «recovery» and new research on long-time effects:
The Council of Evidence-based Psychiatry has given us new knowledge about effects of psychiatric drugs. Recently the Norwegian Psychological Magazin (Tidsskrift for Norsk Psykologforening, Vol 52, nummer 2, 2015, side 126-131) has published an interview with Robert Whitaker. Harrow (4.2, 4.5) showed that the long term recovery rate increases from 5% to 50% after 15 years removing continuous antipsychotic longtime medication. «Relapse after withdrawal of antipsychotic medication is (also) an effect of withdrawal not (just) an effect of sickness (psychosis).» Professor Peter C. Gøtzsche Director of the Nordic Cochrane Centre is publishing books, newspaper articles and gives interviews available also for social media informing about harm done by antipsychotic medication (4.3, 4.4).
Wunderinks randomised studies confirm these results (4.7). «Open dialogue» therapy method uses minimal medication and can reach 80% «revovery» (improvement which allows to come back to family and job) (4.7).
How see critics long term effects and these studies?
5 UN committees (5) have criticised that Norway has violated its human rights commitments because of the highest use of forces treatment in Europe. The Special Rapporteur on Torture Juan E Méndez said 4. March 2013: "States should impose an absolute ban on all forced and non-consensual medical interventions...»
Is there scientific documentation that positive effects of forced medication are so obvious that the «absolute ban» of the Special Rapporteur on Torture is superseded?
Why continues forced medication for patients telling that force medication is experienced «terrible», «cruelly», and «torture».”?
15 years with intentions and programs to reduce forced treatment failed. What can be done? There are experiences of forced treatment banned: Germany without Coercive Treatment in Psychiatry—A 15 Month Real World Experience. What is the reaction of critics of medication free treatment?
Attachment: Experience expertise 2012:3 (Erfaringskompetanse.no 2012:3). Force in Health care. Personnel and dissatisfied patients have different opinions (Tvang i psykisk helsevern. Ansatte og misfornøyde brukeres ulike oppfatninger): http://www.erfaringskompetanse.no/wp-content/uploads/2015/08/Tvang-i-psykisk-helsevern.pdf
UN committees the UN Special Rapporteur on Torture strongly support the patients perspective. Real world experience shows that it is possible to abolish forced treatment. Survivors arguments are supported by the CRPD Committees answer.
5 UN committees (5), Human Rights Commissioner of the Council of Europe, Mental Disability Advocacy Center (MDAC), Ombud against discrimination (LDO), Directorate of Health, Disability organisation support reduction and removal of coercion.
Committee on Economic, Social and Cultural Rights recommends 2013. " that the State party incorporate into the law the abolition of the use of restraint and the enforced administration of intrusive and irreversible treatments such as neuroleptic drugs and electroconvulsive therapy"
Committee against Torture 13 December 2012 CAT/C/NOR/CO/6-7:
(T)he State party should provide systematic, thorough and practical training in the application of the Istanbul Protocol (Manual on Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment) to all relevant health personnel.
The UN Committee against Torture (CAT/C/NOR/QPR/8) asks Norway 2015 preparing Norway’s report for 2016:
(a) “Whether the use of restraints and the enforced administration of intrusive and irreversible treatments such as neuroleptic drugs and electroconvulsive therapy has been abolished in law...
(b) Ensuring that every competent patient, whether voluntary or involuntary, is fully informed about the treatment to be prescribed and given the opportunity to refuse treatment or any other medical intervention... ”
In General Comment 1 premise 42 the CRPD-committee states about force in psychiatry:
“As has been stated by the Committee in several concluding observations, forced treatment by psychiatric and other health and medical professionals is a violation of the right to equal recognition before the law and an infringement of the rights to personal integrity (art. 17); freedom from torture (art. 15); and freedom from violence, exploitation and abuse (art. 16).”
Page 5 of the speech of Special Rapporteur on Torture Juan E Méndez in 22. meeting of the "Human Rights Council" 4. March 2013: "States should impose an absolute ban on all forced and non-consensual medical interventions against persons with disabilities, including the non-consensual administration of psychosurgery, electroshock and mind-altering drugs, for both long- and short- term application. The obligation to end forced psychiatric interventions based on grounds of disability is of immediate application and scarce financial resources cannot justify postponement of its implementation."
Report A/HRC/22/53 of the Special Rapporteur on torture and other cruel, inhuman or degrading treatment of 1. February 2013, Section 32: "For example, the mandate has held that the discriminatory character of forced psychiatric interventions, when committed against persons with psychosocial disabilities, satisfies both intent and purpose required under the article 1 of the Convention against Torture, notwithstanding claims of “good intentions” by medical professionals (ibid., paras. 47, 48)". Section 82.: "The prohibition of torture is one of the few absolute and non-derogable human rights, a matter of jus cogens, a peremptory norm of customary international law."
“Dignity must prevail” – An appeal to do away with non-consensual psychiatric treatment World Mental Health Day – Saturday 10 October 2015 «The concept of ‘medical necessity’ behind non-consensual placement and treatment falls short of scientific evidence and sound criteria.»
«Germany without Coercive Treatment in Psychiatry—A 15 Month Real World Experience»1 shows that considerable improvements are possible. The rate of inpatients under coercive medication fall under 0.5 %. In Norway approx. 10% of inpatients where under coercive medication (SINTEF A26086, ISBN 978-82-14-05679-2)2
The survivors of psychiatry “Bundesverband Psychiatrie-BPE-Germany” asked the UN CRPD committee 19. February 2015: «Please condemn Germany as a human rights criminal. Norway uses approx. 20 times more forced medication compared to Germany. UN CRPD Committee gave concluding observations about the Federal Republic of Germany. Quotes from the States Report of the UN CRPD Committee CRPD/C/DEU/CO/1 on 17/04/2015: 3
«30. The Committee recommends that the State party take all the immediate necessary legislative, administrative and judicial measures to:
(a) Amend legislation to prohibit involuntary placement and promote alternative measures that are in keeping with articles 14, 19 and 22 of the Convention;»
“33. The Committee is deeply concerned that
the State party does not recognize the use
of physical and
chemical restraints, solitary confinement and other harmful practices
as acts of torture.”
Attachments:
Documentation of harm of antipsykotic medication and human rights issues:
4.1. Council of Evidence-based Psychiatry:http://cepuk.org/, http://cepuk.org/unrecognised-facts/long-lasting-negative-effects/
4.2. Psykofarmaka på kort og lang sikt: Tidsskrift for Norsk
Psykologforening, Vol 52, nummer 2, 2015, side 126-131:
https://psykologtidsskriftet.no/intervju/2015/02/psykofarmaka-pa-kort-og-lang-sikt
4.3. PETER C. GØTZSCHE, professor, dr.med., Rigshospitalet: KRONIKEN
5. AUG. 2015 summarises in newspaper Politikken: Tvang i psykiatrien bør forbydes:
http://politiken.dk/debat/kroniken/ECE2781368/tvang-i-psykiatrien-boer-forbydes/
4.4. PETER C. GØTZSCHE, professor, dr.med., Rigshospitalet i Politikken:
'Deadly Psychiatry and Organised Denial' (2015):
4.5. The public mental health system is creating a huge class of chronic
mental patients through forcing them to take ineffective, yet extremely
harmful drugs. http://psychrights.org/Research/Digest/NLPs/neuroleptics.htm
4.6. Effective Non-Neuroleptic Treatment
http://psychrights.org/research/Digest/Effective/effective.htm
4.7 Harrow + Wunderink + Open Dialogue = An Evidence-based Mandate for A New Standard of Care:
4.8. Psych-Drugs Harm - One: Robert Whitaker - A History - September 16, 2015 – CPH
https://www.youtube.com/watch?v=Wd3_Iq8P3Fo
4.9. Jung, E., Wiesjahn, M., Wendt, H., Bock, T., Rief, W. and Lincoln, T.M., 2016. «Symptoms, functioning and coping strategies in individuals with schizophrenia spectrum disorders who do not take antipsychotic medication: a comparative interview study»
Letter to Norwegian Authorities: Norway violates it's human rights obligation to reduce and remove coercion in psychiatry: http://wkeim.bplaced.net/files/UN_coercion.html
16. July 2015: Shadow report: What can be done about NORWAY ranking highest in Europe in use of coercion in psychiatry including human rights breach forced drugging?http://wkeim.bplaced.net/files/150716mdac.html
16. June 2015: Letter to Prime minister Erna Solberg of Norway to respect human rights of people with disabilities and remove coercion in psychiatry http://wkeim.bplaced.net/files/150614pm.html
Legemiddelverket oppfordres å slutte å legitimere helseskadelig langtidsmedisinering med antipsykotika: http://wkeim.bplaced.net/files/150916helsedir.html
Kjetil Lund: 23.JUN.2016 : At all tvangsmedisinering må forbys, slik også FN-komiteen under Konvensjonen om funksjonshemmedes rettigheter og andre FN-organer går inn for, er et nødvendig neste skritt. http://www.aftenposten.no/meninger/debatt/Psykiatri-Uhyggelig-klokkertro-pa-tvangsmedisinering--Ketil-Lund-580997b.html Replikk.
Martin Zinkler: Germany without Coercive Treatment in Psychiatry—A 15 Month Real World Experience: http://www.mdpi.com/2075-471X/5/1/15/htm
1Martin Zinkler. Laws 2016, 5(1), 15; doi:10.3390/laws5010015. Germany without Coercive Treatment in Psychiatry—A 15 Month Real World Experience: http://www.mdpi.com/2075-471X/5/1/15/htm
2Døgnpasienter i psykisk helsevern for voksne (PHV) 20. november 2012, SINTEF. https://www.sintef.no/contentassets/f98d2810156e4dd6b8b7aa1da8174334/endeligrapport_sintef-a26086_2.pdf